
In this section, you can find what evidence-based treatments are most likely to help you.
The following stepped approach may help guide on deciding the best treatment for you.
Listen to world renowned physiotherapist and expert in managing knee cap pain, Professor Kay Crossley (La Trobe Sport and Exercise Medicine Research Centre) discuss surgery, exercise and other treatments for knee cap pain:
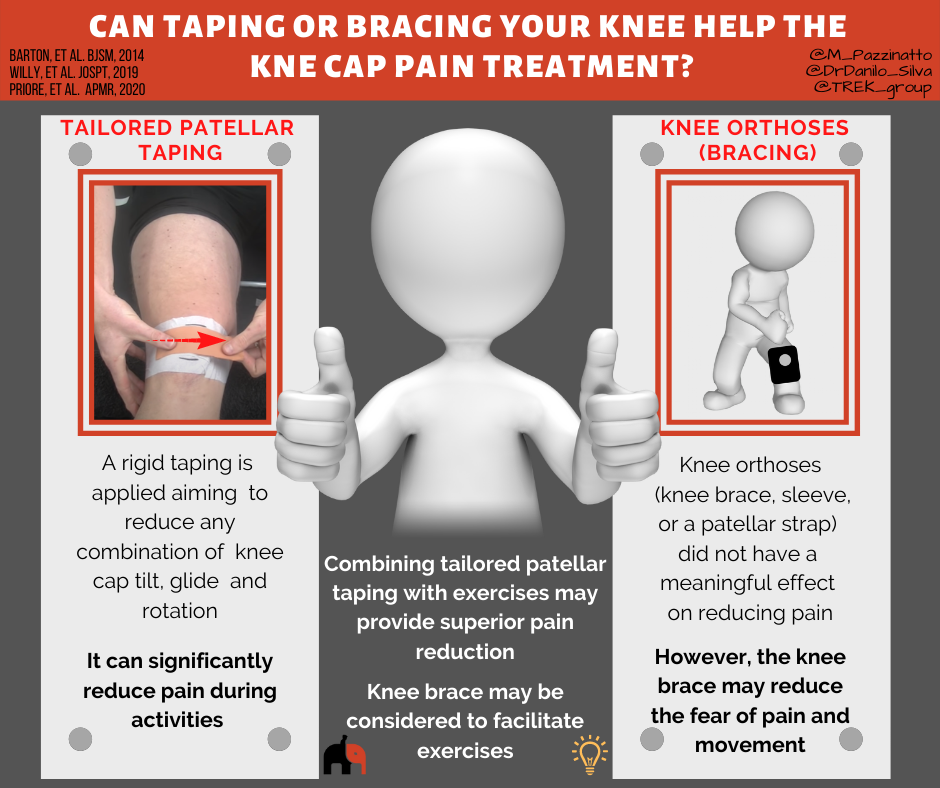
Patellar taping
The most effective way to tape you knee can be different for each person, and research shows that tailoring it to your needs may optimise how much pain reduction you get. You may wish to discuss this with your physiotherapist who can assess your knee and find the most effective way for you.
Based on the best evidence available, the following taping technique may be worth trying:
Importantly, taping techniques are most likely to reduce pain and improve physical function during accompanying exercise program.
Knee Orthoses (Bracing)
Studies revealed that knee orthoses (knee brace, sleeve, or a patellar strap) is not able to reduce pain more than exercise. However, the knee brace may reduce the fear of pain and movement. The use of a knee brace may work as a strategy to improve exercise compliance by reducing fear or even as a mediator to reduce pain and improve physical function.
Additionally, using a medially directed realignment brace while exercising leads to better outcomes in patients with knee cap pain than exercise alone after 6 and 12 weeks of treatment.

Supporting articles
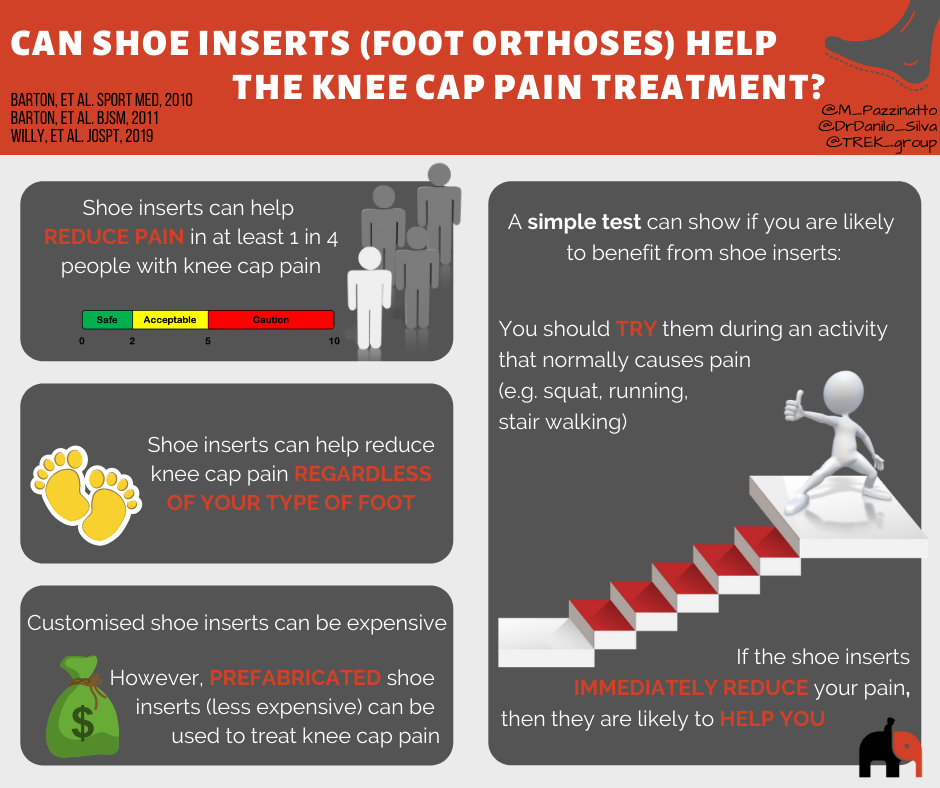
Why might shoe inserts help?

Research suggests that shoe inserts will significantly help reduce pain in anywhere between 25 and 50% of people with knee cap pain over the first 6-12 weeks of treatment. They may also help in the longer term too.
Traditionally, shoe inserts have been provided to people because they have flat (pronated) feet. However, there is a lot of debate about whether this is the right approach. In people with knee cap pain, having flatter feet does not predict strongly whether or not shoe inserts will help. Equally, shoe inserts can help people who are not considered to have flat feet.
A couple of studies have reported that people with flexible feet measured using a specific device are more likely benefit from shoe inserts if they have knee cap pain. This is something you could discuss and assess with the assistance of your physiotherapist or podiatrist.
One of the simplest ways to work out if shoe inserts will help is to try them during an activity that normally causes pain. If the inserts immediately reduce your pain, then they are likely to help. If they do not immediately reduce pain, they are unlikely to help you. It is that simple!
In one study, this test was the strongest predictor of success with shoe inserts given to people with knee cap pain. In the same study, the amount of foot movement (pronation) occurring during walking also predicted success, but not as well.
Aren’t shoe inserts expensive?
If shoe inserts are customised specifically for you by a podiatrist, they can be quite expensive. However, research tells us that this is not necessary for most people with knee cap pain.
Less expensive prefabricated shoe inserts (usually less than $100) can be used to treat knee cap pain. If you complete your rehabilitation exercises given to you by a physiotherapist and get stronger, shoe inserts may only be needed for a short time.
Some physiotherapists have the knowledge and skills to provide you shoe inserts and you should discuss this with the physiotherapist treating you. If not, they can refer you to see a podiatrist to help.
Supporting articles
Barton 2011. Clinical predictors of foot orthoses efficacy in individuals with patellofemoral pain.
Willy 2019. Patellofemoral pain – Clinical practice guideline.
There are a plenty of exercises you could do to improve your knee cap pain, but, some are better than others.
See the video below to choose the more effective exercises.
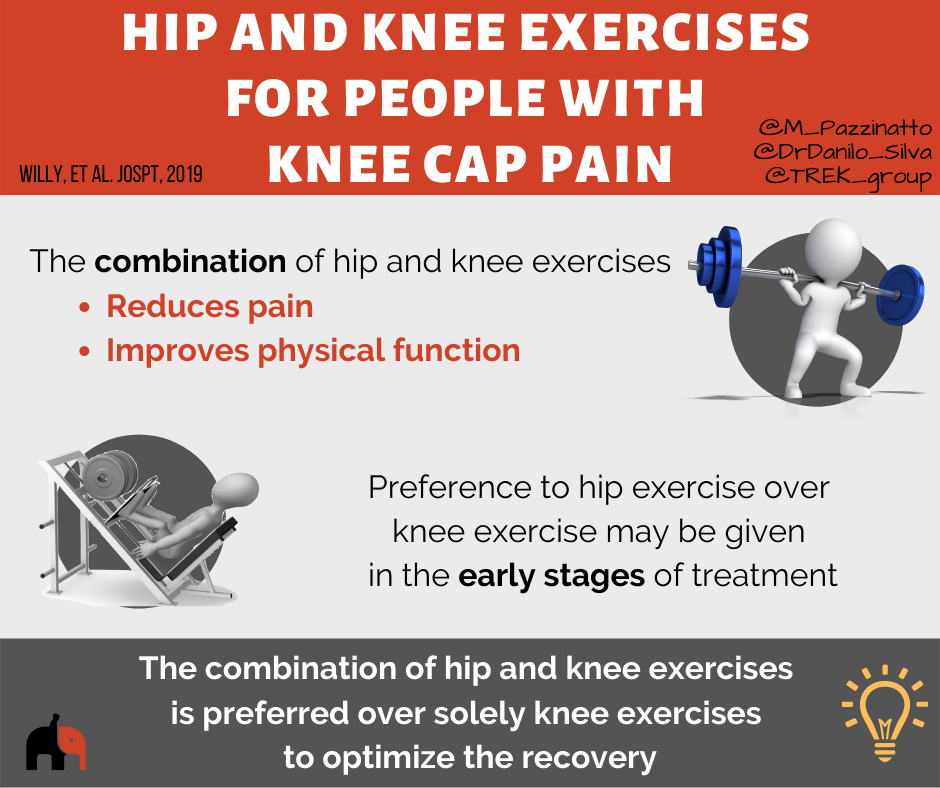
Why is it important to complete exercises targeting my hip muscles?
People with knee cap pain generally have weak and poorly functioning hip muscles.
It is thought that this weakness and poor function may not be the reason as to why you develop pain in the first place. Instead, your hip muscles may become weak because you have changed the way you move, or move less to avoid pain.
Weak and poorly functioning hip muscles are thought to put more stress onto your knee cap during activities like running, walking on stairs and squatting. This is because the muscles can no longer control your thigh well enough, allowing it to roll under the knee cap.
A good way to understand this, is to think of your knee cap as the train, and your thigh as the tracks. If the train (knee cap) moves or tries to derail off the tracks (thigh), this can be because your thigh muscles don’t control the train well enough. However, when the hip is not controlled well enough, the tracks (or thigh) may move underneath the train, having the same derailing effect.
A number of good research trials report that hip targeted exercises are effective in reducing knee cap pain. In the longer term, combining both thigh and hip muscle targeted exercise is the most effective approach to reduce pain.
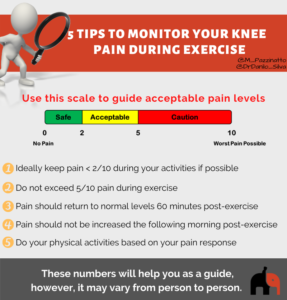
How to monitor your knee cap pain during exercise?
Pain can often cause someone to become fearful of exercise.
However, complete rest is not helpful and it is common for you to have knee cap pain at the beginning of your exercise programs designed to help your knee pain.
If you are completing exercises to help your knee pain, your pain during these should not be higher than you experience during normal activities your perform.
Supporting articles
Barton 2013. Gluteal muscle activity and patellofemoral pain syndrome: a systematic review.
Willy 2019. Patellofemoral pain – Clinical practice guideline.
For your reference, follow the guidance below.
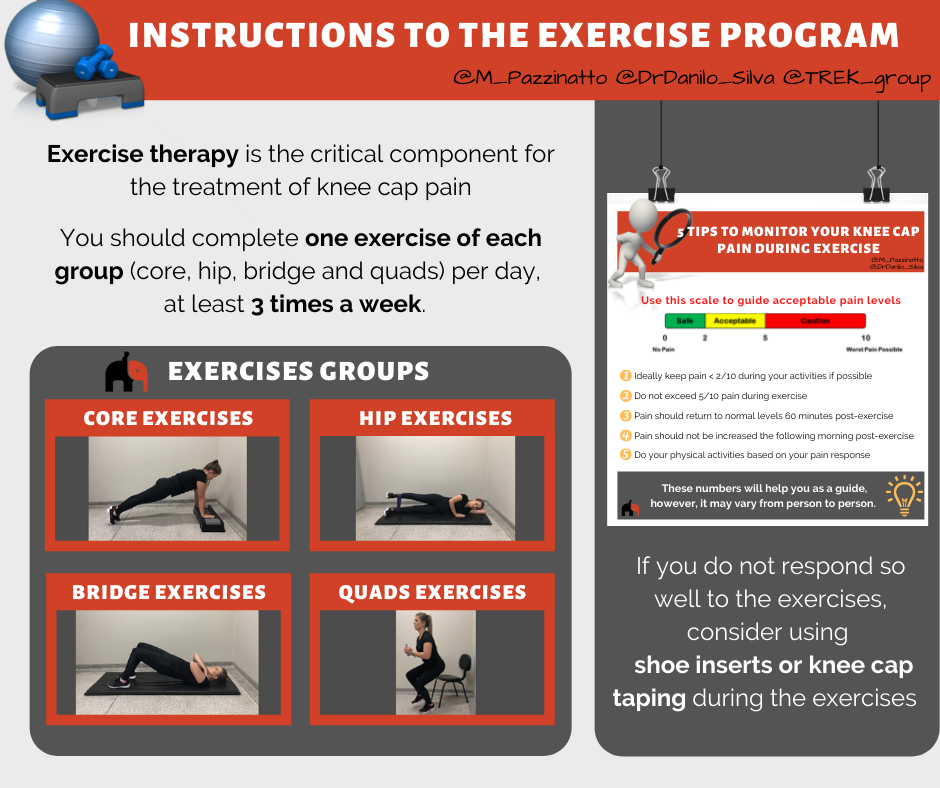
Follow this link to access an exercise program we prepared for you: http://mykneecap.trekeducation.org/what-works/exercise/